
Can Stem Cells Help You Avoid Knee Replacement? What 15 Years of Research Shows
If you are over 40 and your knees ache when you climb stairs, kneel in the garden, or get up after sitting too long, you are not alone. Knee arthritis is one of the most common reasons people slow down, give up activities they love, and start to feel older than they are.
For a long time, the choices felt simple and a little grim: take pain pills, get cortisone shots that wear off, or wait until the knee is bad enough for a total knee replacement. But there is a growing middle path — one that uses your own body’s repair cells to calm the pain, improve how the knee works, and in many people, push a knee replacement years down the road.
Here is what the science actually shows, explained in plain language.
What are “stem cells from your own body”?
Inside your bones is a soft tissue called bone marrow. It is one of the richest sources of your body’s natural repair and signaling cells. When we draw a small amount of this marrow and concentrate it, we get a treatment called bone marrow aspirate concentrate, or BMAC for short.
Think of BMAC as your body’s own repair crew, gathered up and delivered exactly where the damage is. Because it comes from you, there is nothing foreign being added — no donor, no synthetic implant. It is one of the treatments in a field called orthobiologics, which means using the body’s own biology to heal orthopedic problems.
The 15-year question: does it actually last?
A short burst of pain relief is easy. The real question patients ask me is: will it still be helping me years from now?
That is what makes the research from French orthopedic surgeon Dr. Philippe Hernigou so important. His team followed patients with knee arthritis for about 15 years — far longer than most studies — and published the results in the journal International Orthopaedics.
Here is the headline finding. In the group treated with bone marrow cells placed into the bone just beneath the cartilage:
- About 80% still had their own knee at the 15-year mark.
- Only about 1 in 5 went on to need a knee replacement during that time.
- Many had less pain and better knee function that held up over the long term.
To put that in perspective, when the same cells were injected into the joint space alone, the early relief faded — and roughly 70% of those knees eventually needed replacement. Same cells, very different results. The difference came down to one thing: where the cells were placed.
Why where the injection goes changes everything
This is the part most people have never heard, and it is the heart of the matter.
Knee arthritis is not just a cartilage problem. The bone underneath the cartilage — called the subchondral bone — also breaks down and drives pain. If you only treat the joint surface, you miss a major source of the trouble.
That is why the most durable approach targets three areas in the knee, not one:
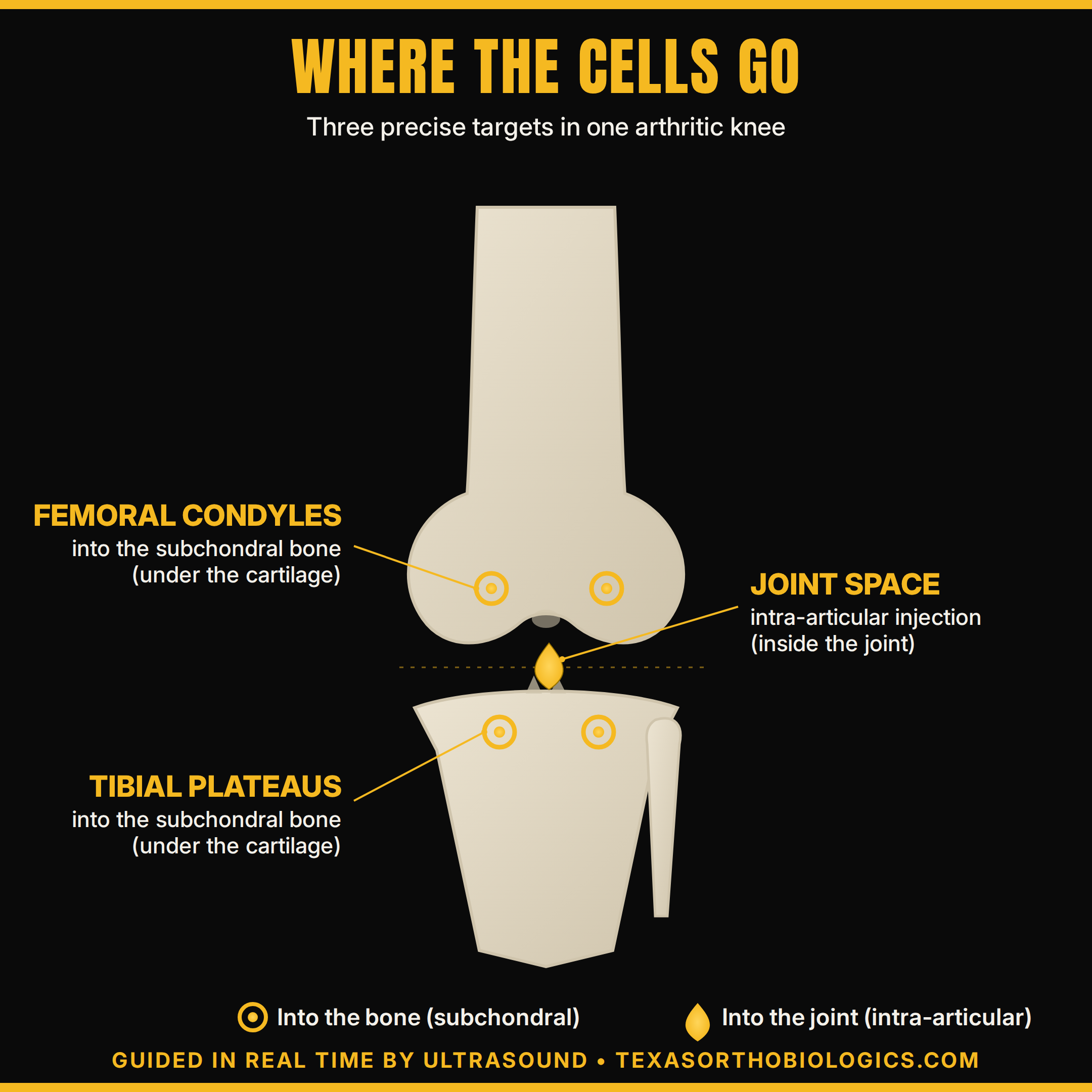
- The femoral condyles — the rounded ends of your thighbone — into the bone just under the cartilage.
- The tibial plateaus — the top surface of your shinbone — again, into the bone under the cartilage.
- The joint space itself — the standard “into the joint” (intra-articular) injection you may already know about.
Placing cells into the bone of the femur and tibia is what gave Dr. Hernigou’s patients results that lasted, while adding the joint-space injection treats the cartilage and lining. Together, they address the whole problem instead of just the surface.
Why ultrasound guidance matters — and why your doctor’s experience matters more
Putting cells into precise spots in living bone is not a “feel for it and hope” procedure. It has to be accurate. That is where ultrasound guidance comes in: real-time imaging that lets me see exactly where the needle is going, so the cells land where they will do the most good — safely and comfortably.
But the tool is only as good as the hands using it. Ultrasound-guided injection is a skill that takes years to master.
I have spent those years — and then some. Since 2008, I have directed the longest-running private training course in musculoskeletal (MSK) ultrasound and orthobiologics, where I have personally trained more than 1,600 physicians in these exact techniques. In other words, when you come to my practice, you are being treated by the doctor who teaches the doctors.
A note on trust
The orthobiologics field is full of bold claims, and it can be hard to know who to believe. I think credentials and leadership in the field matter, so here is where I stand:
- I currently serve as President of the Interventional Orthobiologics Foundation (IOF) — the nonprofit dedicated to setting the standards, ethics, and training for image-guided regenerative injections. interventionalorthobiologics.org
- I serve as Chairman of the Biologic Association — the organization working to unify and advance the responsible use of biologic treatments across medicine. thebiologicassociation.com
These roles mean I am not just using these treatments — I am helping shape how they are done correctly and honestly across the country.
Is this right for everyone?
In a word, no — and any doctor who promises a miracle should give you pause.
BMAC is not a cure for arthritis, and it does not regrow a brand-new knee. Results vary from person to person, and they depend a lot on how advanced the arthritis is. The long-term research is most encouraging for people who still have a reasonable amount of joint space left, which is one more reason not to wait until the knee is bone-on-bone. For some patients, a knee replacement is still the right answer, and I will tell you honestly if that is you.
What BMAC can offer the right patient is a real, evidence-backed option to reduce pain, improve function, and delay or avoid replacement surgery — using nothing but your own cells, placed precisely where they belong.
The bottom line
If you are living with knee arthritis and you are not ready to jump straight to a replacement, you owe it to yourself to understand all of your options. Fifteen years of research suggests that, for the right person, your own body may be one of the most powerful tools available — when the cells are placed in the right targets, by the right hands, with the right guidance.
If you would like to find out whether you are a candidate, I would be glad to take a look.
Serving knee arthritis patients across North Texas
Texas Orthobiologics welcomes patients from throughout the Dallas–Fort Worth Metroplex — including Southlake, Westlake, Plano, Frisco, McKinney, Highland Park, Preston Hollow, Rockwall, and the greater Dallas area. If you are exploring alternatives to knee replacement, we make it easy to schedule a consultation from anywhere in DFW.
References
- Hernigou P, Delambre J, Quiennec S, Poignard A. Human bone marrow mesenchymal stem cell injection in subchondral lesions of knee osteoarthritis: a prospective randomized study versus contralateral arthroplasty at a mean fifteen year follow-up. Int Orthop. 2021;45(2):365-373. doi:10.1007/s00264-020-04571-4
- Hernigou P, Bouthors C, Bastard C, Flouzat Lachaniette CH, Rouard H, Dubory A. Subchondral bone or intra-articular injection of bone marrow concentrate mesenchymal stem cells in bilateral knee osteoarthritis: what better postpone knee arthroplasty at fifteen years? A randomized study. Int Orthop. 2021;45(2):391-399. doi:10.1007/s00264-020-04687-7
This article is for general education and is not medical advice. Regenerative treatments are not a guaranteed cure, results vary, and they are not appropriate for every patient or every stage of arthritis. Please consult a qualified physician to discuss whether these options are right for your specific situation.

Comments